
Thyroidectomy, the surgical removal of the thyroid gland, is a common treatment for thyroid cancer and certain benign thyroid conditions. Following thyroidectomy, careful monitoring is crucial to detect any recurrence or complications. Among the various imaging modalities available, ultrasound and computed tomography (CT) scans are frequently employed. This article will delve into a comparison of ultrasound and CT scans in the context of post-thyroidectomy care, outlining their respective strengths and limitations for effective monitoring.
Ultrasound: The Primary Imaging Tool for Post-Thyroidectomy Follow-Up
Ultrasound is often the first-line imaging modality recommended for post-thyroidectomy surveillance. This is largely due to its non-invasive nature, lack of ionizing radiation, cost-effectiveness, and accessibility. Ultrasound excels at visualizing the soft tissues of the neck, including the thyroid bed (the area where the thyroid gland was removed) and the surrounding lymph nodes.
Advantages of Ultrasound in Post-Thyroidectomy Monitoring:
- High Resolution for Soft Tissues: Ultrasound provides excellent detail of superficial soft tissues, allowing for the detection of small nodules or masses in the thyroid bed or enlarged lymph nodes that may suggest recurrence. It is particularly effective at identifying the characteristic features of papillary thyroid carcinoma, the most common type, which often presents as hypoechoic nodules and may contain punctate calcifications.
- No Radiation Exposure: Unlike CT scans, ultrasound does not use ionizing radiation, making it safe for repeated use during long-term follow-up, particularly important for younger patients.
- Cost-Effective and Widely Available: Ultrasound is generally less expensive than CT scans and is widely available in most healthcare settings, facilitating routine and frequent monitoring.
- Real-time Imaging and Dynamic Assessment: Ultrasound allows for real-time imaging, enabling the operator to assess the area dynamically and guide fine-needle aspiration cytology (FNAC) if a suspicious nodule is detected.
Limitations of Ultrasound:
- Limited Penetration: Ultrasound waves do not penetrate bone well and are limited in their ability to visualize deeper structures in the neck or areas behind bone.
- Operator Dependent: The quality of ultrasound images and interpretation can be influenced by the skill and experience of the sonographer and radiologist.
- Less Effective for Distant Metastases: Ultrasound is primarily focused on the neck and is not designed to evaluate for distant metastases in the chest or other parts of the body.
CT Scan: When is it Necessary After Thyroidectomy?
Computed tomography (CT) scans utilize X-rays to create detailed cross-sectional images of the body. While not typically the first-line choice for routine post-thyroidectomy follow-up, CT scans play a valuable role in specific clinical scenarios.
Advantages of CT Scans in Post-Thyroidectomy Monitoring:
- Superior Visualization of Deeper Structures and Bone: CT scans provide excellent visualization of deeper structures in the neck, mediastinum (chest cavity between the lungs), and bones. This is particularly useful for assessing for extrathyroidal extension or invasion into surrounding tissues, which might not be fully evaluated by ultrasound.
- Detection of Distant Metastases: CT scans of the chest, abdomen, and pelvis can be performed to evaluate for distant metastases in patients at higher risk of recurrence or when there is clinical suspicion of distant spread.
- Assessment of Airway and Esophagus: CT scans can provide detailed information about the trachea (windpipe) and esophagus, which can be important in cases of locally advanced thyroid cancer or to evaluate for complications.
Limitations of CT Scans:
- Radiation Exposure: CT scans involve ionizing radiation, which, although generally low in modern scanners, is a consideration, especially for repeated scans.
- Lower Resolution for Soft Tissues Compared to Ultrasound: While CT scans provide excellent anatomical detail, their soft tissue resolution is generally not as high as ultrasound for superficial structures in the neck.
- Higher Cost and Less Accessibility: CT scans are more expensive than ultrasounds and may be less readily available in all settings, potentially delaying routine monitoring.
- Contrast Dye Risks: CT scans often involve intravenous contrast dye to enhance image detail. Contrast dye can carry risks of allergic reactions and kidney problems, especially in individuals with pre-existing kidney disease.
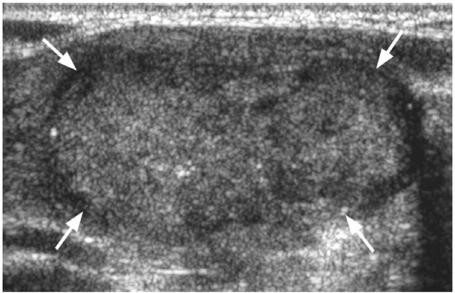 Ultrasound of solid hypoechoic follicular thyroid cancer (arrows).
Ultrasound of solid hypoechoic follicular thyroid cancer (arrows).
Ultrasound vs. CT: Choosing the Right Imaging Modality After Thyroidectomy
In routine post-thyroidectomy follow-up for differentiated thyroid cancer (papillary and follicular thyroid cancer), neck ultrasound is generally the preferred initial imaging modality. Its ability to effectively visualize the thyroid bed and neck lymph nodes, combined with its safety, cost-effectiveness, and accessibility, makes it ideal for regular surveillance.
CT scans are typically reserved for specific situations, including:
- Suspected Distant Metastases: When there is clinical suspicion or risk factors for distant metastases, CT scans of the chest, abdomen, and pelvis are valuable for staging and monitoring.
- Evaluation of Extrathyroidal Extension: In cases of locally advanced thyroid cancer or when ultrasound findings are inconclusive regarding extrathyroidal extension, CT scans can provide more detailed information about invasion into surrounding structures.
- Preoperative Planning for Re-operation: If recurrence is suspected and surgical re-excision is considered, CT scans can assist in surgical planning by providing a comprehensive anatomical roadmap.
- Follow-up of Medullary or Anaplastic Thyroid Cancer: While ultrasound is still used, CT scans may play a more prominent role in the follow-up of less differentiated thyroid cancers like medullary and anaplastic thyroid cancer, which have a higher propensity for distant spread.
Conclusion
Both ultrasound and CT scans are valuable imaging tools in post-thyroidectomy care. Ultrasound serves as the cornerstone for routine follow-up due to its excellent soft tissue detail in the neck, safety, and cost-effectiveness. CT scans are strategically used in specific scenarios, particularly when evaluating for distant metastases or assessing deeper structures and extrathyroidal extension. The choice between ultrasound and CT scan, or their combined use, should be guided by individual patient risk factors, clinical findings, and the specific type of thyroid cancer. Consultation with an endocrinologist and radiologist is crucial to determine the most appropriate imaging strategy for optimal post-thyroidectomy monitoring.
